Why pain in children needs its own chapter
Adult first aid usually treats pain as a symptom that the casualty reports — "where does it hurt", "how bad is it out of ten", "what does it feel like" — and the response is shaped by the answers. Pain in children is harder. A toddler cannot rate their pain on a 1-to-10 scale, an infant cannot describe what hurts, and a school-age child may say "fine" because they want to keep playing or they are worried about getting into trouble. The educator has to read the body, the behaviour, and the situation as well as listen to the words. G9.2.9
Pain is also often the first sign that a child has a condition that needs attention — an injury they have not described, an infection that is brewing, a chronic illness that is flaring. The educator who takes a child's pain seriously is often the one who catches the underlying problem early enough to make a difference.
This chapter is about general pain recognition and management. The pain that comes with specific conditions has its own chapters — fractures and sprains in the fractures and sprains chapter, bleeding wounds in the bleeding chapter, burns in the burns chapter, and so on. This chapter is about pain as a phenomenon and a clinical sign in its own right.
§ Instructor's note
The teaching point of this chapter is that children's pain is real, often undertreated, and an important diagnostic clue when something is wrong. The historical assumption that children "do not feel pain like adults" is wrong, and the historical practice of denying analgesia to children because they could not describe the pain is now recognised as harmful. Drill the rule: believe the child, look at the body, comfort first, and refer when you are not sure what the pain is telling you.
The myth that children do not feel pain the same as adults
For most of the twentieth century, medical practice underestimated and undertreated pain in children. Surgery on infants was sometimes performed without adequate analgesia on the assumption that infants could not feel or remember pain. Children's reports of pain were dismissed as exaggeration or attention-seeking. The pendulum has swung in recent decades, and current practice — including paediatric first aid — recognises that:
- Children feel pain at least as keenly as adults, and possibly more so. The neural pathways for pain are present from birth.
- Infants and very young children have less capacity to modulate their pain response than older children or adults, meaning they can be more overwhelmed by it.
- Children remember pain, particularly the older preschool and school-age groups, and unmanaged pain in childhood can have lasting effects on later medical experiences.
- Children are not exaggerating when they report pain. Their reports are usually accurate to their experience.
- Pain is an important clinical sign in children just as in adults — it is the body telling the carer that something is wrong.
The educator who takes a child's pain seriously is doing both the kind thing and the clinically correct thing.
How children show pain
Children at different ages express pain in different ways, and the educator's recognition needs to fit the age:
Infants and very young toddlers
Infants and pre-verbal toddlers cannot describe pain in words, so they show it through:
- Crying — often a high-pitched, inconsolable cry that is different from the hungry or tired cry. Carers who know the child can usually tell the difference.
- Facial expression — eyes squeezed shut, brow furrowed, mouth open in a wide grimace, lips tight. Pain expressions in infants are recognisable to anyone who looks for them.
- Body posture — drawing up the legs, arching the back, stiffening, holding a part of the body still or guarded.
- Clinginess — wanting to be held, refusing to be put down, crying when separated from a familiar adult.
- Refusing to eat or drink — particularly relevant in babies, where refusal of feeds can be one of the few signs that something is wrong.
- Changes in sleep — disturbed sleep, unable to settle, waking more often than usual.
- Reduced movement of an affected part — a baby who will not use one arm, or who cries when their leg is moved during a nappy change.
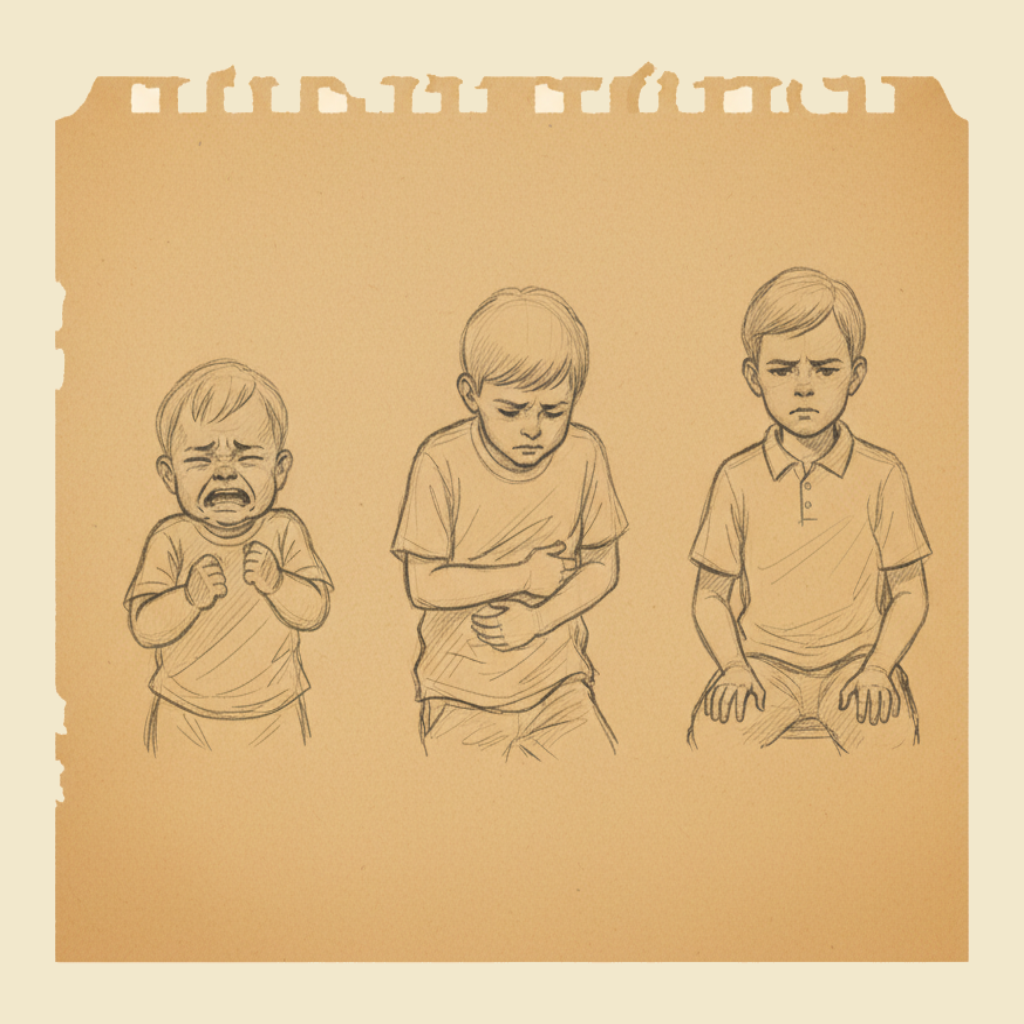
Young children (2 to 5 years)
Young children have some words but limited ability to localise or describe sensation:
- Saying "it hurts" without being able to say where, why, or how much.
- Pointing to a part of the body — sometimes accurate, sometimes not. A child who points to their tummy may have abdominal pain, or may have learned that "tummy" is what you say when you want attention.
- Crying or whimpering — often less dramatic than an infant, but persistent.
- Withdrawal — going quiet, sitting alone, refusing to join in.
- Regressive behaviour — wanting comfort items, thumb-sucking, asking for a parent, asking to be carried.
- Refusing favourite activities — a child who does not want to play with their favourite toy, eat their favourite snack, or do their favourite thing has either lost interest or is in pain.
- Holding or rubbing the affected part, or holding still and refusing to move it.
- Crying or fussing during specific activities — getting changed, walking, sitting, lying down.
School-age children (5 to 12, in OOSH care)
Older children can describe pain more accurately, but with caveats:
- They can describe location, quality, and intensity — "it hurts here, it's a sharp pain, it's a 7 out of 10".
- They can use a pain scale — number scale, faces scale, colour scale. Most paediatric services use the Wong-Baker FACES scale (a row of cartoon faces from happy to crying) for children who cannot use numbers reliably.
- They may underreport — particularly if they think describing the pain will get them sent home, separated from friends, or in trouble. Children who are afraid of medical attention may downplay their symptoms.
- They may overreport — particularly if they are seeking attention, want to get out of an activity, or are upset about something else and are using "it hurts" as the available vocabulary. This is not malingering; it is the child reaching for the response they need.
- Body language is still important — even an older child whose words say "I'm fine" but whose body says "I'm protecting this leg" is in pain.
The educator's job is to listen, look, and combine the two. The words tell you part of the story; the body tells you the rest.
Assessing the pain
A simple framework for assessing a child's pain at the service:
- Where is the pain? Ask the child to point if they can. Look for guarding or holding.
- When did it start? Sudden onset (usually injury or acute event) vs gradual (usually inflammation or illness).
- What was the child doing when it started? A fall, a particular activity, eating, after a sting?
- What does the pain feel like? Sharp, dull, throbbing, burning. Older children can answer this; younger ones may not.
- How bad is it? Scale of 1 to 10 for older children; FACES scale for younger; observation of behaviour for the youngest.
- What makes it better or worse? Movement, position, pressure, distraction.
- Are there any other symptoms? Fever, vomiting, swelling, redness, bleeding, change in colour, change in alertness.
- Does the child have a known condition that might explain the pain — a chronic illness, a recent injury, an allergy, a recent vaccination?
- How is the child's general condition? Alert, engaged, breathing normally, normal colour, behaving as usual — or any deterioration in the broader picture?
This is not a medical history; it is enough information to form a sensible impression and to communicate accurately with the parents and (if needed) the medical staff.
Pain that points to something serious
Most pain in a child at the service is from a minor injury, a normal developmental complaint, or a simple infection. Some patterns of pain point to something more serious and need urgent attention:
- Severe sudden abdominal pain, particularly with vomiting, fever, refusal to move, or guarding the abdomen. Could be appendicitis, intussusception, a hernia, or other surgical conditions.
- Severe headache, particularly with vomiting, fever, confusion, neck stiffness, or photophobia. Could be meningitis or other serious neurological problem.
- Severe chest pain — uncommon in children but always serious.
- Pain after a fall from height or any significant impact, particularly with a change in alertness, vomiting, or visible deformity.
- Pain in a limb that the child will not use — possible fracture, severe sprain, infection.
- Pain combined with a non-blanching rash — possible meningococcal disease. See the fever chapter.
- Pain combined with breathing difficulty — could be a cardiac problem, severe respiratory illness, or chest injury.
- Pain combined with reduced level of consciousness — could be many things, all serious.
- Pain from a known dangerous mechanism — a snake or spider bite, a marine creature sting, a serious burn.
- Pain that is much more severe than the visible injury — a small wound with disproportionate pain may indicate something deeper that has not been recognised.
Any of these is a parent phone call at minimum, and an ambulance for the more severe cases. The principle is: if the pain seems out of proportion to what you can see, or if it is accompanied by any other red flag, escalate.
Severe or sustained abdominal pain in a child is a symptom that should never be dismissed as "tummy ache" without assessment. The list of serious causes — appendicitis, intussusception, testicular torsion in boys, ovarian torsion in girls, bowel obstruction, severe constipation — is real, and the consequences of missing one are significant. If a child has severe abdominal pain that is not improving, is worsening, is accompanied by fever, vomiting, or refusal to move, or is much worse than what would be expected from any obvious cause, contact the parent immediately and recommend medical assessment. When in doubt, escalate to the ambulance.
What an educator can do for pain
The educator's pain management toolkit at the service is mostly non-pharmacological — comfort, distraction, positioning, ice packs, reassurance. The drug interventions are the parent's and the doctor's responsibility, except where specific medications are authorised on the child's medication form. What the educator can offer:
Comfort
The single most effective pain intervention an educator has is closeness with a familiar adult. A child in pain often wants to be held, sit on a lap, or be near a trusted person. Provide that. Sit with the child, hold them if they want to be held, speak softly. The presence of a calm adult reduces the child's distress and, through the distress, the experienced intensity of the pain.
Distraction
Distraction is a real and well-evidenced pain intervention in children. The brain has a limited attention budget, and giving it something else to focus on reduces the share of attention that goes to the pain. Effective distractions:
- Reading a book to the child.
- Counting, singing, or reciting nursery rhymes together.
- Looking at pictures in a book or on a phone.
- Telling a story.
- Describing what is happening in the room.
- Playing a simple game the child knows and enjoys.
- Asking the child to focus on their breathing ("can you take three slow deep breaths with me?") — works particularly well with school-age children.
The distraction should be calm, gentle, and engaging — not high-energy or chaotic. The goal is to draw the child's attention away from the pain without overstimulating them. See the communication and distraction chapter for more on the technique.
Positioning
The right position for a child in pain depends on where the pain is:
- Abdominal pain — let the child curl up if they want to. Forcing them to lie flat or stand up usually makes it worse.
- Back pain — let the child find their own position.
- Limb pain — support the limb in a comfortable position with a pillow, a folded towel, or your hands. Do not force movement.
- Headache — quiet dim space, head supported, lying down or sitting, whichever the child prefers.
- Chest pain — sitting up is usually more comfortable than lying down.
- Generalised illness pain — let the child find their own position.
The general rule is to follow the child's lead. They will adopt the position that hurts least.
Cold and warmth
For many injuries, cold is helpful — it reduces swelling, slows the inflammatory response, and provides some pain relief through numbing. A cold pack wrapped in a thin cloth (never directly on the skin), applied for 10 to 15 minutes at a time, is the standard for sprains, bruises, and bumps. See the fractures and sprains chapter for the technique.
For some pains — abdominal cramps, back pain, sore muscles — warmth is more comforting than cold. A warm (not hot) wheat bag or hot water bottle wrapped in a cloth can help. Test the temperature on your own forearm before applying to a child to avoid burns.
Wound care
For pain from a wound, the standard wound care — clean, cover, support — also reduces pain by protecting the area from movement, contamination, and air contact. See the minor wounds chapter.
Communication
Telling the child what is happening, in age-appropriate language, reduces the fear that often accompanies pain. "I'm going to put a cold pack on your knee for a few minutes — it will feel cold but it will help your knee feel better" is more reassuring than silent application of an unfamiliar object. Children who know what to expect cope better than children who are surprised.
Pain medication
Paracetamol and ibuprofen are commonly used for pain in children at home, but the educator does not administer them at the service unless the medication has been authorised on the child's medication form, with parental consent and appropriate dosing instructions. The reasoning is the same as for fever — see the fever chapter.
If a child needs analgesia beyond what comfort and ice can provide, the right answer is to phone the parent and let them decide whether to come and collect the child or to authorise medication on the spot. For a child with a chronic condition who has a standing authorisation for analgesia (e.g. a child with juvenile arthritis whose parents have signed a medication form), the educator follows the plan.
Aspirin is never given to children under 16 with fever or viral illness because of the risk of Reye syndrome — see the fever chapter.
The chronic-pain child
A small proportion of children at the service have chronic conditions that involve ongoing or recurrent pain — juvenile arthritis, sickle cell disease, severe migraine, recurrent abdominal pain syndromes, and others. These children typically have:
- A diagnosis that the parents have shared with the service.
- A medication plan with specific instructions for pain management at the service.
- An action plan for what to do during a flare or pain episode.
- Particular triggers or warning signs that the educators should know about.
The educator's job is to know which children at the service have chronic pain conditions, where their plans are, and what to do when a flare happens. This is the same general approach as for any chronic condition — see the emergency action plans chapter.
A child with chronic pain is not "exaggerating" when they report a flare. Their pain is real and may be more frequent or severe than other children's. Believe them, follow the plan, communicate with the parents, and provide comfort.
When pain becomes a child safety concern
Occasionally, pain or injury in a child raises a concern about possible abuse or neglect. The pattern that should prompt thinking includes:
- Injuries in unusual locations — soft tissue of the face, neck, ears, abdomen, genital area, inner arms or thighs.
- Injuries that do not match the explanation — bruising in shapes that suggest particular objects, burns in patterns suggesting deliberate contact, fractures in non-mobile children.
- Injuries of different ages — bruises at different stages of healing.
- Inconsistent stories about how the injury happened, particularly if the story changes.
- Delays in seeking medical attention for significant injuries.
- The child's fear or reluctance to talk about the injury or about the people who care for them.
- A pattern across multiple incidents rather than a single event.
Child safety concerns are managed through the service's child protection policy and, in most jurisdictions, mandatory reporting laws that apply to educators. If you have a concern, escalate to the nominated supervisor immediately. Do not investigate yourself, do not interrogate the child, and do not delay. The reporting framework is the education and care state regulations chapter — mandatory reporting is state law and varies by jurisdiction.
This is mentioned here because pain assessment is often the moment when a concern surfaces. The pain assessment is the everyday activity; the safeguarding response is the rare but serious escalation.
A child with intellectual disability, autism, communication difficulties, or sensory processing differences may express pain in ways that are unfamiliar or counterintuitive. They may not say "it hurts", may not make eye contact, may not seek comfort in the usual way, or may show pain through behaviours that look like agitation, withdrawal, or aggression. The educator's job is to know the child, to know how they normally behave, and to take any change from their normal as a possible sign of pain or distress. The parents and any therapy team are the source of information about how a particular child shows pain.
Documenting and communicating
A child who has had pain at the service deserves a written record of:
- The time, location, and nature of the pain.
- The presumed cause (if known).
- The assessment (severity, associated signs).
- What was done about it (comfort, ice, position).
- The response (improved, unchanged, worsened).
- The communication with the parent.
- Any escalation (medical advice, ambulance, hospital).
The parent should be told the same information, in conversation, at pickup or by phone. The educator's communication should be honest, specific, and forward-looking: what happened, what was done, how the child is now, what to watch for.
Pain in children should be recognised, taken seriously, and managed with non-pharmacological measures including comfort, positioning, distraction, and the appropriate application of cold or warmth. Pharmacological pain relief is administered only under specific authorisation and according to the child's prescribed plan. Pain that is severe, is out of proportion to the visible injury, is accompanied by other red-flag signs, or is affecting a child's general wellbeing should prompt prompt medical assessment. The first aider should always communicate honestly with the child and the parents about the assessment, the response, and the next steps.
What not to do
- Do not dismiss a child's report of pain because they are young, easily distracted, or have been complaining about something else recently.
- Do not assume an infant or non-verbal child does not feel pain just because they cannot describe it.
- Do not force a child to move, stand, or do anything that obviously increases their pain. Let them adopt the position they prefer.
- Do not apply a cold pack directly to skin — wrap it in a cloth.
- Do not apply heat that has not been temperature-tested.
- Do not give paracetamol or ibuprofen without specific authorisation on the medication form.
- Do not give aspirin to a child under 16. Ever.
- Do not ignore severe abdominal pain, severe headache, pain after a significant impact, or pain combined with other red flags.
- Do not investigate a possible safeguarding concern alone — escalate to the nominated supervisor.
- Do not forget to comfort the child while you do the technical things. Comfort is a real intervention.
You will rehearse pain assessment in role-play scenarios — an infant who cannot speak, a toddler with limited vocabulary, a school-age child who is downplaying their symptoms — and practise the comfort and distraction techniques that are the educator's main tools. The instructor will also discuss the recognition of pain patterns that point to more serious problems and the escalation pathway when one of those patterns appears.
Children feel pain, children remember pain, and children's pain is often the body's way of telling the carer that something needs attention. Believe the child, look at the body, comfort first, and take the time to think about what the pain might mean. Most pain in a child at the service has a simple cause and a simple response; the cases that don't deserve the educator's curiosity, escalation, and refusal to dismiss. Hold the child, explain what is happening, follow the plan if there is one, and call the parent when you are unsure.
— ANZCOR Guideline 9.2.9 (heat-related illness, with general paediatric first aid principles)