Why breathing difficulty is the leading paediatric emergency
In adults, the most common medical emergencies are cardiac. In children, they are respiratory. Children's airways are smaller, their respiratory reserve is lower, and the most common pathway to a paediatric cardiac arrest is not a primary heart problem — it is hypoxia from a respiratory problem that was not recognised or not treated in time. Get the breathing right and you have prevented most paediatric collapses; miss it, and you are racing the clock to a cardiac arrest that could have been avoided. G9.2.3 G9.2.4
This chapter is about the general recognition of breathing difficulty in children — the signs that something is wrong with the airway or the lungs, the spectrum from mild to severe, and the immediate response. The specific conditions that produce breathing difficulty have their own chapters: asthma is in the asthma chapter, anaphylaxis is in the anaphylaxis chapter, choking is in the choking chapter, and drowning is in the drowning chapter. All of those produce breathing difficulty, and the recognition signs are the same across all of them.
§ Instructor's note
The teaching point is the recognition pattern. Children compensate for respiratory trouble for a long time before they crash, and when they crash they crash fast. The job is to spot the compensation while it is still happening, not to wait for the crash. Drill the rule: fast breathing, hard work to breathe, noisy breathing, change in skin colour, change in level of consciousness — any one of these is a red flag, and any combination is an emergency.
The way a healthy child breathes
Knowing what normal looks like is the foundation for noticing what abnormal looks like. A healthy child:
- Breathes quietly. You should not be able to hear the breathing across the room.
- Breathes evenly. The chest rises and falls rhythmically, without pauses, gasps, or extra effort.
- Breathes through the nose most of the time, with the mouth closed at rest.
- Has pink, well-perfused skin — lips, fingertips, ears, gums all the same warm tone as the rest of the face.
- Is alert and engaged, behaving appropriately for their age and the situation.
The normal respiratory rate is age-dependent. Approximate ranges:
- Infants under 1 year: 30 to 60 breaths per minute. Infants breathe fast.
- Toddlers (1 to 3 years): 24 to 40 breaths per minute.
- Preschoolers (3 to 6 years): 22 to 34 breaths per minute.
- School-age (6 to 12 years): 18 to 30 breaths per minute.
You do not need to count breaths in every interaction; the rates are useful as a calibration. What matters operationally is the pattern — fast for the child, slow for the child, irregular, laboured, noisy.
The signs of respiratory distress
A child with breathing difficulty shows one or more of the following. The more signs you see, and the more severe they are, the more urgent the situation:
Increased respiratory rate
The first compensation a child makes for any respiratory problem is to breathe faster. A child whose normal rate is 25 breaths per minute and is now breathing at 45 is working harder than they should be, even if they look otherwise OK. Tachypnoea (the medical word for fast breathing) is the earliest and most consistent sign.
Increased work of breathing
A child who is struggling will use accessory muscles — muscles that are not normally needed for breathing — to move air. The visible signs:
- Nasal flaring — the nostrils flare outward with each breath, particularly visible in infants.
- Tracheal tug — the soft tissue at the base of the throat is sucked in with each breath.
- Intercostal recession — the skin between the ribs is sucked inward with each breath.
- Subcostal recession — the skin under the ribs is sucked inward.
- Sternal recession — the breastbone itself is sucked in (in young children with flexible chest walls this is dramatic).
- Head bobbing in infants — the head moves forward and back with each breath.
- Use of shoulder muscles — visible in older children who are visibly heaving the shoulders to breathe.
These signs collectively are called increased work of breathing and they indicate that the normal effort of breathing is no longer enough. The harder the work, the more severe the distress.
Noisy breathing
Normal breathing is silent. Noises mean something is interfering with airflow:
- Stridor — a high-pitched sound on inspiration (breathing in), indicating obstruction in the upper airway (throat, larynx, trachea). Croup, anaphylactic upper-airway swelling, and inhaled foreign bodies all produce stridor.
- Wheeze — a whistling or musical sound, usually on expiration (breathing out), indicating narrowing of the lower airways (bronchi). Asthma is the classic cause.
- Grunting — a soft "uhh" sound at the end of each expiration, particularly in infants. Grunting is the child's instinct to hold a small amount of pressure in the lungs and is an ominous sign of respiratory failure.
- Cough — productive or dry, persistent or paroxysmal. Cough by itself is not always an emergency, but a cough combined with other distress signs is significant.
Posture changes
A child in respiratory distress often adopts a tripod position — sitting upright, leaning forward, hands on knees or on the ground in front, head extended. This position maximises the use of the accessory muscles and is a sign that the child is working hard to breathe. Toddlers may become unusually still and quiet, refusing to lie down because lying down makes breathing harder.
Skin colour changes
- Pallor — a pale, washed-out appearance, often with a slight grey or blue tinge.
- Cyanosis — a blue tinge to the lips, the tongue, the fingernail beds, the earlobes. Central cyanosis (around the lips and mouth) is a late and serious sign of severe hypoxia. By the time you can see it, the child has been struggling for some time.
- Mottling — a patchy, marbled appearance to the skin.
Changes in level of consciousness
- Restlessness, agitation, anxiety — early. The child knows something is wrong and the brain is responding to falling oxygen with increased adrenergic drive.
- Quietness, withdrawal, drowsiness — later and worse. A child who was crying and now has stopped, or who was anxious and now seems calm, has not necessarily improved — they may be deteriorating. A drowsy child in respiratory distress is in serious trouble.
- Loss of consciousness — pre-arrest. Imminent collapse.
Unable to talk in full sentences
An older child who can normally chat in full sentences but is now speaking in single words, or is too short of breath to talk at all, has significant distress. Listen for the rhythm of speech as well as the words.
Drooling
A child who is drooling because they cannot manage their own saliva — particularly with the head extended forward — has an upper airway problem that may be obstructing swallowing as well as breathing. This can be a sign of severe upper airway swelling and is an emergency.
The "early" versus "late" signs
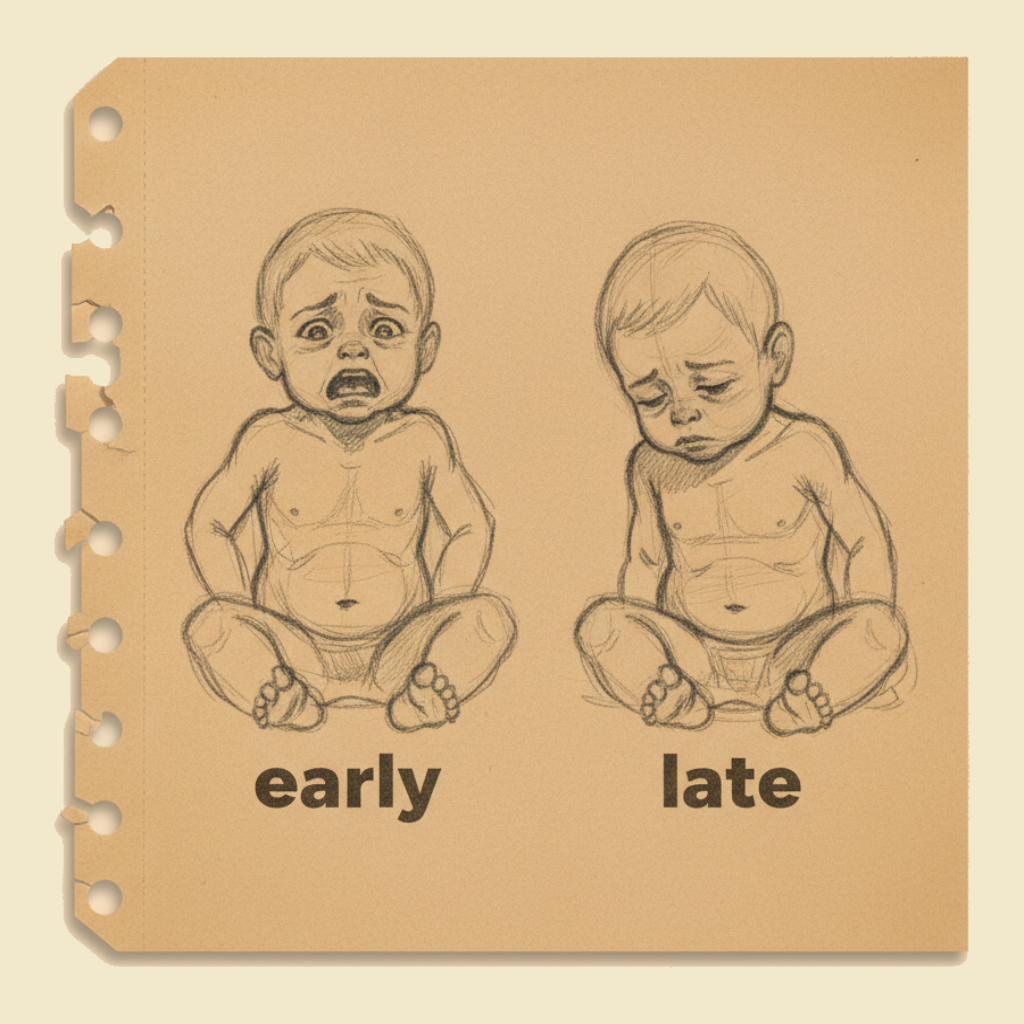
The recognition framework that matters most is the difference between early and late signs of respiratory distress, because the late signs are warnings that cardiac arrest is imminent.
Early signs (still compensating):
- Mild to moderate tachypnoea
- Mild work of breathing (some recession, some nasal flaring)
- Restlessness, anxiety
- Cough, mild wheeze, mild stridor
- Skin colour still normal or slightly pale
- Still talking, still alert
Late signs (decompensating, getting close to arrest):
- Very fast or, paradoxically, slowing respiratory rate
- Severe work of breathing, exhaustion, the child unable to maintain the effort
- Quietness, drowsiness, reduced responsiveness
- Cyanosis (especially central — around the lips)
- Grunting in infants
- Inability to talk
- Drooling, head-extension posture
A child with late signs is in respiratory failure and is heading for cardiac arrest within minutes. Call 000 immediately, get any reversible cause treated (give the EpiPen if anaphylactic, give the puffer if asthmatic, clear the airway if obstructed), and prepare to start CPR if the breathing stops.
A child with early signs is the situation in which good first aid can change the outcome. Treat the underlying cause (asthma puffer, EpiPen, comfortable upright positioning, oxygen if available, calm reassurance) and watch closely for any progression. Many children will improve. Some will not, and you have to be ready to escalate.
Counter to instinct, a child who has been wheezing and crying and is now quiet has not necessarily got better. A quiet, drowsy, exhausted child in respiratory distress is closer to arrest, not closer to recovery. Do not be reassured by the silence. The child who is screaming and pink is doing better than the child who is quiet and pale. If a child you have been worried about suddenly goes quiet, escalate immediately.
The general approach to a child with breathing difficulty
The first aider's response, before getting into condition-specific protocols:
- Recognise the distress and decide on the urgency. Early signs need treatment and observation; late signs need an immediate ambulance.
- Call for help — another educator to assist, the nominated supervisor, and 000 if the situation warrants it. Do not wait until the child is in arrest before calling. If in doubt, call early — the call can always be downgraded.
- Position the child for comfort. Most children with respiratory distress prefer to sit upright. Do not force a child with breathing difficulty to lie down — this often makes them worse. Let them adopt the position they find easiest.
- Look for and treat any obvious cause.
- If they have a known condition with an action plan (asthma, anaphylaxis), follow the plan. Find the puffer, find the EpiPen, give the medication.
- If they may have inhaled or swallowed a foreign body, follow the choking protocol — see the choking chapter.
- If they have visible swelling of the face, lips, or tongue, treat as anaphylaxis even without a confirmed allergy history.
- Reassure the child and stay calm. Anxiety makes breathing difficulty worse — both for the child and through the contagious effect of an anxious adult on a frightened child. Speak calmly, sit at the child's level, do not crowd them, and explain in simple words what is happening.
- Monitor closely. Watch the work of breathing, the colour, the level of alertness, the talking. Look for any deterioration. A child who is improving should be visibly improving within minutes of treatment; a child who is not improving needs the next level of care.
- Be ready to escalate. Have a phone ready, have someone who knows how to call 000, and know where the nearest defibrillator is. The goal is not to need them, but to be ready if the situation worsens.
- Document everything — time of onset, signs observed, treatments given, response to treatment, outcome — for the parent, the ambulance, and the incident record.
When to call 000
Call 000 for any child with:
- Severe respiratory distress — heavy work of breathing, exhaustion, late signs.
- Cyanosis — blue lips, tongue, or fingernail beds.
- Stridor — particularly stridor that is new, getting worse, or accompanied by drooling.
- Severe wheeze or asthma not responding to puffer within a few minutes.
- Suspected anaphylaxis — any breathing change in a known or suspected allergic exposure.
- Foreign body suspected to be in the airway that has not been cleared.
- Reduced responsiveness or drowsiness in any child with breathing difficulty.
- Any child whose breathing difficulty is unexplained and not improving.
When in doubt, call. The dispatcher can advise, the ambulance can be cancelled if it turns out not to be needed, and the time you save by calling early is the time the child needs. See the accessing emergency services chapter for the details of the call.
Common causes of breathing difficulty in children
For first-aid purposes, the most likely causes in an ECEC setting are:
- Asthma — the most common cause of recurrent breathing difficulty in children. Treated with the child's own puffer in line with the action plan. See the asthma chapter.
- Anaphylaxis — sudden onset, often with skin signs (hives, swelling) and a known allergen exposure. Treated with the child's own EpiPen. See the anaphylaxis chapter.
- Choking on a foreign body — sudden onset, usually during eating or play with small objects. Back blows and chest thrusts. See the choking chapter.
- Croup — viral upper airway swelling, classic seal-bark cough and stridor, usually worse at night. Sit the child upright, keep calm, and seek medical assessment.
- Bronchiolitis — viral lower airway inflammation in infants, with wheeze and increased work of breathing. Common in babies under 1 year in winter.
- Pneumonia or bronchitis — bacterial or viral infection, usually with fever and a few days of progressive symptoms.
- Inhalation of smoke, fumes, or vomit — accidental exposures, water inhalation in the drowning chapter, and similar.
The first aider does not need to make the medical diagnosis. The job is to recognise the distress, treat any obvious reversible cause, and escalate to medical care for everything else.
A crying or upset child often has fast, irregular, and dramatic-looking breathing — but they are not in respiratory distress; they are emotional. The way to tell the difference: an upset child still has normal skin colour, can settle if comforted, can talk in sentences when calm, and has no other signs of distress. A child in genuine respiratory difficulty has the work-of-breathing signs even when they have stopped crying, has skin colour change, and does not improve with reassurance. Use the clinical signs, not the volume of distress, to make the call.
After the immediate response
If the child improves with treatment and no longer needs emergency care, they still need a follow-up plan. A child with even a mild episode of respiratory distress at the service should:
- Have the parents informed promptly with a clear description of what happened.
- Be observed closely for the rest of the session for any return of symptoms.
- Be referred for medical assessment, even if the immediate episode has settled. A first attack of asthma, a first allergic reaction, or a child whose existing condition has just escalated all warrant medical review.
- Have the incident documented in the service's incident, injury, trauma and illness record.
If the child needed an EpiPen or needed the ambulance, they also need to go to hospital for observation regardless of how well they look afterwards. See the referral and ambulance response chapter for the rationale.
The recognition of respiratory distress in infants and children is the cornerstone of paediatric first aid. Signs include increased respiratory rate, increased work of breathing (nasal flaring, recession, accessory muscle use), abnormal noises (stridor, wheeze, grunting), changes in skin colour, and changes in level of consciousness. Late signs — exhaustion, slowing rate, cyanosis, drowsiness — indicate impending respiratory failure and the need for immediate emergency care. The first aider should treat any reversible cause, support the child in a comfortable position, call emergency services for severe distress, and be prepared to commence resuscitation if the child becomes unresponsive and is not breathing normally.
What not to do
- Do not wait for cyanosis before calling 000. Cyanosis is a late sign.
- Do not be reassured by a child who has gone quiet after being noisy. The silence may mean exhaustion, not improvement.
- Do not force a child in respiratory distress to lie down. Let them adopt the position they find easiest.
- Do not try to look down the throat of a child with stridor and drooling — this can worsen the obstruction. Refer to medical care urgently.
- Do not withhold a child's own action plan medication out of caution. The puffer or the EpiPen is what the plan is for.
- Do not delay calling 000 because you are not sure if the situation is "serious enough". Err on the side of calling early.
- Do not crowd or restrain a child with breathing difficulty — both make it worse.
- Do not leave the child unattended while waiting for the ambulance. Stay with them, monitor, and be ready to start resuscitation if they deteriorate.
You will rehearse the recognition of paediatric respiratory distress on a manikin and on role-play scenarios — spotting the early and late signs, distinguishing genuine distress from emotional upset, deciding when to escalate, and walking through the response for a child with asthma, anaphylaxis, and croup. The technical interventions (puffer, EpiPen, calm positioning) are simple; the recognition is the part that benefits most from practice with the experienced eye of an instructor.
Children in respiratory difficulty give you warning signs, and the warning signs are the moment to act — before the late signs arrive and the situation is no longer recoverable with simple first aid. Look for fast breathing, hard breathing, noisy breathing, colour changes, and changes in alertness. Treat the obvious causes, position the child for comfort, call early when you are worried, and never be reassured by a child who has gone quiet. Most paediatric resuscitations start with a respiratory problem that someone did not catch early enough; the educator who catches it is the one who keeps it from becoming a resuscitation.
— ANZCOR Guideline 9.2.4 (paediatric airway and breathing)