The headline rule
If a child or infant is in cardiac arrest — unresponsive, not breathing normally, no signs of life — the answer is CPR and an AED, the same as for an adult. The AED is suitable for any age, the algorithm is the same, and the only differences are the pad placement and (where they are available) the use of paediatric pads or a paediatric energy setting. Hesitation about whether the AED is "for children" causes preventable deaths; the AED is for the casualty in front of you, regardless of how old they are. G7
In an education and care setting, paediatric cardiac arrest is rare but not impossible. The most common causes in this age group are respiratory in origin — choking, drowning, severe asthma, anaphylaxis, infection — rather than the primary cardiac causes that dominate in adults. The shockable rhythms (ventricular fibrillation, pulseless ventricular tachycardia) are less common in children than in adults, but they do occur, and when they do, the AED is the only intervention that reverses them. The first aider's job is to recognise cardiac arrest, start CPR, and get the AED on the child as fast as possible.
This chapter is about the specifics of using an AED on a child or infant. The basics of AED operation, the four-step process, and the safety considerations that apply to any AED use are in the aed safety and maintenance chapter, and the underlying CPR techniques are in the cpr techniques topic. The general "AED is for everyone" reasoning applies to children just as it does to adults — see also the chain of survival chapter.
§ Instructor's note
The teaching point is that there is no age-based exclusion from defibrillation. Educators new to first aid often have an instinct that the AED is "too much" for a small child, the way you would not give an adult-strength medication to a toddler. The AED is not like a medication; it is a rhythm-detector and shock-delivery device that decides for itself whether a shock is appropriate. If the rhythm is shockable, the shock is needed regardless of size. Drill the rule: any age, any size — start CPR, attach the pads, follow the prompts.
When to use an AED on a child
The criteria are exactly the same as for an adult:
- The child is unresponsive — no response to voice or touch.
- The child is not breathing normally — no normal breathing, agonal gasps only, or no breathing at all.
- CPR is in progress — chest compressions and rescue breaths in line with paediatric technique.
- An AED is available — yours or one nearby (most education and care services have one on site, and ACECQA encourages their installation).
If all four are true, the AED goes on. Do not stop CPR while the AED is being prepared, except for the brief pauses the machine prompts you to take. The CPR is the intervention that keeps blood moving to the brain; the AED is the intervention that may restore the rhythm.
Cardiac arrest in children is most often the result of something else — usually a respiratory event — and the underlying cause may need attention as well as the cardiac arrest itself. But the immediate response is the same: CPR, AED, ambulance, in parallel.
Paediatric pads versus adult pads
Most modern AEDs ship with two sets of pads: adult pads (large, for casualties over 8 years old or above 25 kg) and paediatric pads (smaller, for children up to 8 years old or below 25 kg). Paediatric pads do two things:
- They are physically smaller, so they fit on a child's chest without overlapping.
- They are wired or coded so that the AED delivers a reduced energy dose appropriate for a smaller body. The exact mechanism varies by manufacturer — some have a separate paediatric pad set, some have a "paediatric mode" key the responder turns, some have a switch on the device itself. The result is the same: a lower-energy shock.
If paediatric pads are available, use them on a child up to 8 years old or under 25 kg. They are the manufacturer's intended option for that age group.
What to do if no paediatric pads are available
This is the most important point in the chapter, and the one most often misremembered: if paediatric pads are not available, use the adult pads on a child. Do not delay defibrillation because the right pads are not in the AED case. Adult pads on a child are unequivocally better than no defibrillation, and the energy of an adult shock — while higher than the paediatric setting — is not so high that it causes meaningful harm to a child in cardiac arrest who would otherwise die.
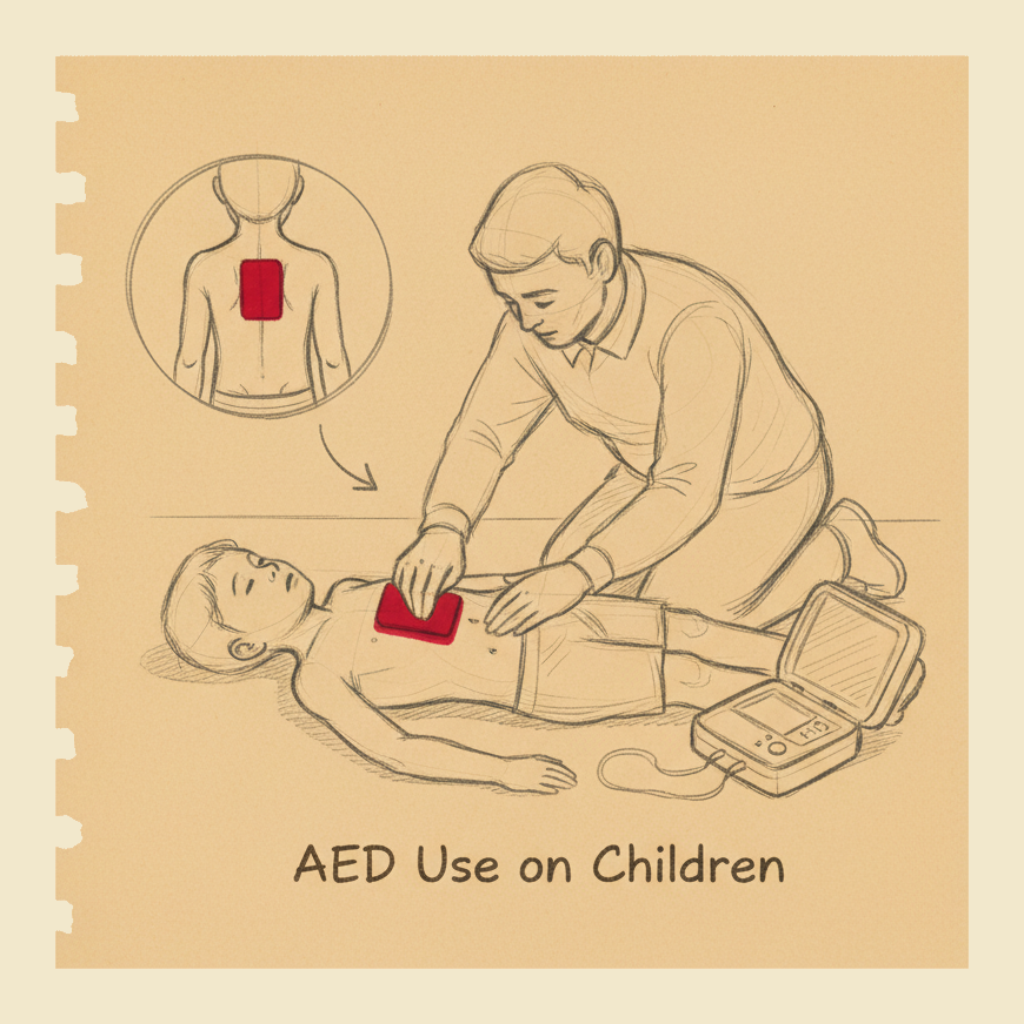
The pad placement on a small child or infant with adult pads needs slight adjustment: the pads should not touch each other or overlap. On a small chest there may not be room to place the adult pads in the standard right-upper-chest / left-side-of-ribcage position, in which case the right answer is to place one pad on the front of the chest and one pad on the back — the anterior-posterior placement. One pad goes in the centre of the chest over the heart, the other goes on the back directly behind it. The result is the same effective shock delivery, with no risk of the pads contacting each other.
The single rule to remember is: if the only pads available are adult pads, use them rather than not defibrillate at all. The opposite — paediatric pads on an adult — is not recommended because the energy dose is too low to be reliably effective on an adult heart. But adult pads on a child is acceptable when nothing else is available.
If you are about to defibrillate a child and the AED has only adult pads, use the adult pads. Do not pause to look for paediatric pads, do not wait for someone to bring a different machine, do not skip the AED altogether. Cardiac arrest is fatal in minutes; the right pads are a refinement, not a precondition. Adult pads on a child have saved children's lives. No pads on a child has saved nobody.
Pad placement on a child
For a child between roughly 1 and 8 years old, with paediatric pads (or adult pads where the chest is large enough), the standard placement is:
- One pad on the upper right chest, just below the collarbone, to the right of the breastbone.
- One pad on the left side of the chest, on the lower ribcage at the side, just below the armpit.
This is the same placement as for an adult and works as long as the two pads do not touch each other.
For a small child or infant where the chest is too small to accommodate two pads side by side without overlap, switch to the anterior-posterior placement:
- One pad on the centre of the chest over the breastbone, between the nipples.
- One pad on the centre of the back, directly behind the chest pad, between the shoulder blades.
The child needs to be turned briefly to apply the back pad. CPR is paused while the pads are applied — the same way it would be for an adult — and resumed immediately afterwards.
The pads must be in good skin contact: dry the skin if it is wet or sweaty (a quick wipe with a towel or piece of clothing), shave any thick chest hair (rare in children, common in adolescents), and remove any clothing or jewellery that would interfere. If the child is wearing a metallic adornment that touches the pad area, move it before applying the pad.
Pad placement on an infant
For an infant under 1 year old, the same principles apply with the modifications:
- Use paediatric pads if available. Adult pads are too large for an infant's chest in the standard placement and the anterior-posterior placement is required.
- Anterior-posterior placement is the default. One pad on the front of the chest in the centre, one pad on the back directly behind. The infant's small body makes side-by-side placement impractical.
- Use whatever pads are available if paediatric pads are not — the same rule applies as for older children.
The history of infant defibrillation is short — for many years there were no AEDs designed for infants, and the practice was uncertain — but current ANZCOR guidelines support AED use in infants when an AED is available, particularly with paediatric pads, and accept the use of adult pads in anterior-posterior placement when nothing else is available.
The most important point: cardiac arrest in an infant is overwhelmingly secondary to a respiratory cause, so the primary intervention is prompt and high-quality CPR with effective rescue breaths, and the AED is the supporting intervention rather than the lead one. But "supporting" does not mean "skip" — if a shockable rhythm is present, only the AED can correct it.
The four-step process — same as for an adult
The actual process of using the AED on a child is the same as for an adult:
- Switch the AED on. Most AEDs power up with a single button or by opening the lid. Once on, the device begins talking to you with voice prompts.
- Attach the pads to the child's bare chest, in the placement appropriate to their size and the pads available. Follow the diagram on the pads themselves; every pad set has a picture showing where it goes.
- Follow the AED's voice prompts. The AED will analyse the rhythm — during which it asks everyone to stand clear of the casualty so the analysis is not corrupted by movement — and then tell you whether a shock is advised or not.
- Deliver the shock if advised, by pressing the flashing button (or, on a fully automatic AED, by standing clear and letting the device fire on its own). After the shock, the AED prompts the resumption of CPR for two minutes, then re-analyses.
If the AED says no shock advised, that does not mean the casualty is fine — it means the rhythm is not one that defibrillation can correct. Resume CPR immediately, follow the AED's prompts for the next analysis, and continue until the ambulance arrives or the casualty shows signs of life.
Stand clear and the safety considerations
The safety rules for AED use on a child are the same as for an adult:
- Stand clear during analysis — do not touch the child while the AED is analysing the rhythm. Movement and contact corrupt the analysis.
- Stand clear during shock delivery — the shock travels through the child's chest and any conductive contact with another body. Loud, clear "stand clear, shocking now" before pressing the button.
- Remove the child from any wet surface if possible — a puddle, a wet floor, a swimming pool surround. Move the child onto a dry area before applying the pads. If that is not possible, dry the chest area thoroughly and proceed.
- Remove any metal jewellery that touches the pad area or the pad path.
- Do not place pads over a medication patch, an implanted device (rare in children but possible), or a recent surgical scar. Move the pad to an alternative location nearby.
For more on these safety considerations, see the aed safety and maintenance chapter.
A small number of children have implanted cardiac devices — pacemakers, defibrillators — usually because of congenital heart disease. The presence of an implanted device is visible as a lump under the skin near the upper chest. If you can see one, place the AED pad at least 8 cm away from the device, or use the anterior-posterior placement to keep the pads off the implant. The AED is still appropriate; the pad position is the only thing that needs adjusting.
After the shock — and after the casualty recovers
If the AED delivers a shock and the child shows signs of life — moving, breathing, opening eyes — leave the pads attached, place the child in the recovery position if they are unresponsive but breathing, and wait for the ambulance. The AED will continue to monitor and may deliver another shock if the rhythm becomes shockable again.
If the AED delivers a shock and the child does not show signs of life, resume CPR immediately. The AED will prompt another analysis after two minutes. Continue the cycle.
If the child fully recovers — breathing normally, alert, responsive — they still need to go to hospital. A cardiac arrest in a child is a serious event with a serious underlying cause, and the child needs full medical assessment regardless of how well they look afterwards. Do not let the parents take the child home from the service "now that they're fine"; the ambulance is the right answer.
The community AED — and your service's AED
Many education and care services have an AED on site. ACECQA encourages this and many state Regulatory Authorities recommend it as part of best-practice safety arrangements. If your service has one, you should know:
- Where it is — usually mounted on a wall near the entrance or in a staff area.
- How to access it — most AED cabinets are unlocked or have a simple-release alarm.
- Whether it has paediatric pads — and where they are stored if not immediately on the device.
- How to switch the device on and follow the prompts — practice with the trainer at face-to-face training so you have done it at least once.
- The maintenance schedule — battery and pad replacement dates, who is responsible.
If your service does not have an AED, the nearest community AED — at a school, shopping centre, sports facility, or AED-registered location — may be reachable in time for a cardiac arrest at your service. The AED's location is worth knowing, and the chain of survival chapter discusses why every minute matters.
A word about shock energy
For the technically curious: the standard adult AED delivers a biphasic shock at around 150 to 200 joules. A paediatric pad set or paediatric mode reduces the dose to roughly 50 to 75 joules — calibrated to the smaller mass of a child's heart. The reduced dose is safer for the smaller heart but is still effective at converting a shockable rhythm.
When adult pads are used on a child because nothing else is available, the child receives an adult-energy shock. The risk is myocardial injury from the higher-than-ideal dose, but the alternative is death from the unconverted rhythm. The risk-benefit calculation is unambiguous: take the higher-dose shock over no shock. Children have survived adult-energy defibrillation many times. Children who were not defibrillated because the right pads were not available have not.
This is the underlying reason for the rule: never let the absence of paediatric pads stop you from defibrillating a child. The drug dose analogy that might tempt you — "I would not give an adult dose of paracetamol to a toddler" — does not apply. The AED is not a medication; it is an electrical intervention with a small therapeutic window and a clear binary effect. The dose-precision concerns of paediatric pharmacology do not translate.
Automated external defibrillators may be safely and effectively used on children of any age, including infants. Where available, paediatric pads or a paediatric energy attenuator should be used for children under 8 years old or under 25 kg. Where paediatric pads are not available, adult pads should be used rather than withholding defibrillation. Pad placement on a child or infant may be in the standard sternum-apex configuration where the chest is large enough, or in the anterior-posterior configuration where the chest is small. The decision to use an AED on a child should not be delayed by uncertainty about the appropriate pad type.
What not to do
- Do not withhold an AED from a child because paediatric pads are not available. Use adult pads.
- Do not delay starting CPR while the AED is being prepared. CPR is the constant; the AED is layered on top of it.
- Do not allow the pads to touch each other or overlap on a small chest. Switch to anterior-posterior placement instead.
- Do not place pads over a patch, implant, or recent surgical scar. Move the pad to an adjacent location.
- Do not touch the child during analysis or during shock delivery. Stand clear and call it loudly so others stand clear too.
- Do not use paediatric pads on an adult — the energy dose is too low to be reliably effective.
- Do not stop CPR after a successful shock if the child is still not showing signs of life. Resume immediately.
- Do not let the family take a recovered child home. The hospital assessment is essential.
You will rehearse AED use on a paediatric manikin, with both a paediatric pad simulation and an "adult pads only" scenario where you have to switch to anterior-posterior placement. You will also practise the call-out and stand-clear sequence so it is in your muscle memory. The trainer device looks and behaves like a real AED but does not deliver shocks; the practice is in the timing and the choreography, not the electrical part.
An AED is suitable for a child of any age, including an infant, and the same machine you would use on an adult is the right machine for a child in cardiac arrest. Paediatric pads if you have them; adult pads if you don't; anterior-posterior placement if the chest is small. The rule to remember is that the absence of the perfect option is never a reason to skip defibrillation altogether. Start CPR, attach the AED, follow the prompts. Any age, any size, the same answer.
— ANZCOR Guideline 7 (automated external defibrillation)